The International Society of Ultrasound in Obstetrics and Gynecology (ISUOG) has recently published guidance on the use of personal protective equipment (PPE) and other methods to reduce the hazard of SARSCoV2 infection for clinicians and sonographers undertaking ultrasound examinations1,2
The documents, however, clearly state that guidance in relation to PPE differs from country to country and region to region and that local guidance should be followed when this is available. This document attempts to fill that space in the context of heterogeneity and varied education level, economic status and cultural beliefs and practices in India.
As in the ISUOG document, it is emphasized at the outset that many of the measures suggested in this document are based on limited research and evidence. This advice is drawn from various sources available from China3,4, Hong Kong5, Singapore6, United Kingdom7,8, Canada9,
continental Europe10,11,12,13 the USA14,15and the WHO16. It is a list of recommended practices that are so far believed to be the most effective methods for reducing the transmission of SARSX CoVX2 between patients and healthcare providers.
Important Considerations
Respiratory droplets from coughing, sneezing, loud conversation, and direct contact are responsible for the spread of SARSCoV2. This happens when body fluids touch another person’s eyes, nose or mouth, or an incision, laceration, or abrasion). The disease caused by the virus has been named COVID19.
Evidence suggests that healthcare workers must use appropriate PPE, even if they remain further than 1 meter away from asymptomatic patient17.
It is very much possible that carriers may be asymptomatic. It would be prudent, therefore, to presume that every patient and attendant is a potential source of infection.
Precautions need to extend way beyond the lockdown period and cannot stop even if the incidence curve of COVID19 flattens or falls.
Precautions, tact, knowledge and security measures will be put to test as soon as the lockdown is lifted. There will be a massive patient overload & being prepared is the only answer in this situation.
This document is a guidance note and not a compulsory protocol. Every institution/clinic can have a modified protocol to enhance protection.
An institution/clinic can opt to remain closed for services as long as the regional law does not enforce the Essential Services Maintenance Act
Contents of this Statement
This document includes the following:
Peculiarities of an Ultrasound Examination that potentially threaten the Healthcare Professional
Indications for performing Ultrasound Scans during the pandemic
Patient Scheduling
Patient Evaluation at First Point of Patient Contact, Triaging and appropriate PPE
Informed Consent
Venue Sanitation and Rearrangement
Equipment Sanitation
Accelerating Availability of Final Reports
Advance Resourcing of Protective Devices and Materials
Staff Education
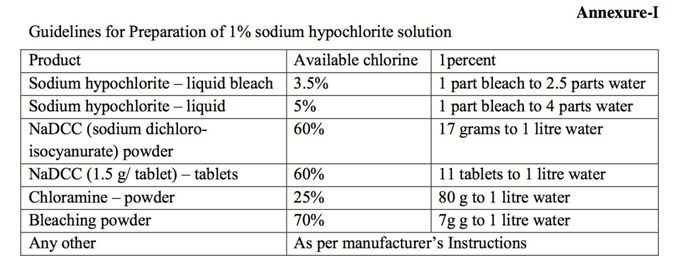
Annexure 1: Methods of preparing a 1% sodium hypochlorite solution
Annexure 2: COVID19 Specific Patient Declaration & Informed Consent and Release form
Threats to Healthcare Professionals During an Ultrasound Examination
The ultrasound examination has multiple aspects that can increase transmission from the patient to the healthcare worker and vice versa1,17 including:
Small examination rooms
Absent or restricted natural ventilation
Closed vent and central (single cooling source, multiple outlet) air conditioning without HEPA filtration
Insufficient distancing between patient and examiner
Long examination times
Transvaginal and invasive procedures
Coughing, sneezing, loud conversation, anxious deep breathing and sighing by the patient and attendant
Repeated handling of transducers, machine desktops, keyboards, touch screens, trackball, and recording devices .
Indications for performing Ultrasound Scans
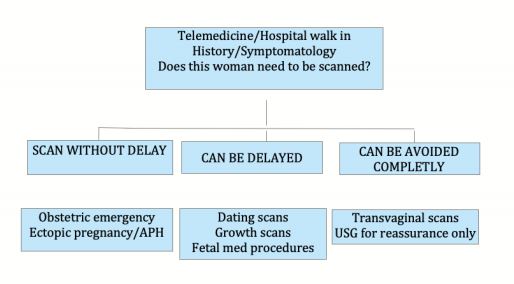
Considering the inevitable reduction in resources and capacity, which limits the number of scan appointments available, based on ISUOG guidelines it is recommended that appointments should be triaged to one of the following three categories:
The following indications may be considered:
Dating scans between 6X10 weeks should be postponed and dating should be done at the Early Morphology 11 weeksX13 weeks 6 days scan window.
Patients with bleeding per vaginum or pain need appointment prioritization. Bleeding score can be assessed based on pictorial graphs; soakage of 3 pads in an hour would designate as a score of 3.
The Anomalies Scan at 18X20 weeks may be delayed by a few weeks. Even under pandemic circumstances, it is likely that a patient will be able to obtain permission from a District Court along with a Medical Board Opinion for delayed termination in case of a major/lethal anomaly.
Second-trimester scans should be given priority over first trimester scans
“Routine” Growth and Doppler scans should be postponed to a 36 weeks assessment. If the pandemic recedes, these can be rescheduled earlier
“Decision Making” Growth and Doppler scans between 28X41 weeks should be considered on priority. Information from this scan dictates time, place and mode of delivery and this decision may be critical to save lives of mothers and fetuses.
The 36 weeks Growth and Doppler scan is a useful triaging tool for early delivery decisions and may need to be carried out although FIGO recommends clinical assessment and delivery during a pandemic.
The above-mentioned prioritization will need to be modified depending on the extension of the lockdown.
Patient Scheduling
This aspect is critical for the safety of patients, physicians & clinic staff. Adherence to these suggestions will ensure social distancing.
Advance Scheduling is necessary and walk-in patients are to be discouraged. This should be carried out on the phone by experienced staff.
The gap between appointments will vary from institution to institution and should be based on
Staff numbers
Availability of waiting spaces
Availability of scanning rooms
Type of scan
Turn around time from the arrival of the patient to exit.
Patient Evaluation at First Point of Patient Contact, Triaging and appropriate PPE
This should ideally be carried out on the phone at the time of scheduling an appointment or else when the patient arrives at the clinic.
For hospital walk-ins, the latter option becomes even more important and must be followed at the time of patient arrival.
Recording the temperature is an ideal screen but cumbersome and impractical: handheld non-contact forehead thermometers are in short supply and patients are using paracetamol and not always being truthful.
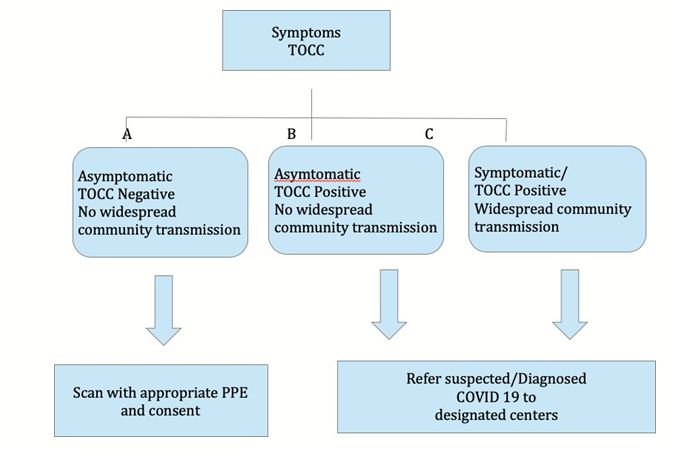
A history of travel, occupation, contact, and cluster (TOCC) is recommended1. Experienced staff should be deputed to handle this and a formal form may be used (Annexure 2)
Travel should include a detailed itinerary, transit locations and date of return
Occupation should be asked as a direct question
A history of exposure to a test positive case should be directly asked for
A history of living in a known positive cluster or visiting such a cluster should be noted
A properly filled declaration and written informed consent document should be obtained from the patient (Annexure 2).
Patients can then be triaged into one of three categories1:
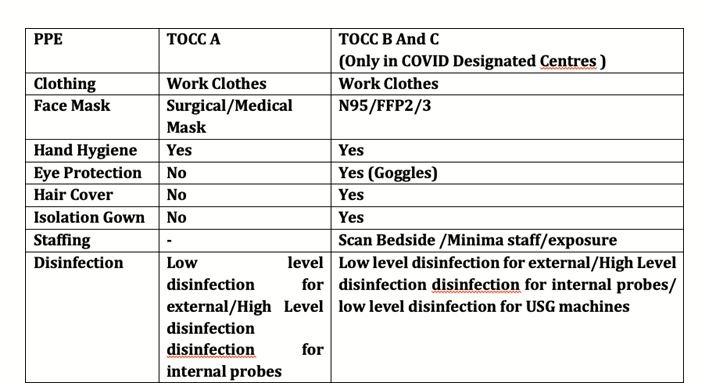
Based on this categorization, the following PPE should be utilized:
Informed Consent
Informed written consent should be taken from the woman, explicitly stating that she understands that there is a risk of her getting infected by visiting any place during this pandemic and that she also knows that the ultrasound scan needs to be done at this stage (Annexure 2).
Venue Sanitation and Rearrangement
The following recommendations apply to sanitation1,13,18,19,20 and logistics. The WHO16,21 and Ministry of Health and Family Welfare, Government of India recommendations18 are particularly useful in this regard.
Physical barriers, such as glass or plastic windows panels, should be used to reduce exposure to the COVID19 virus. This approach can be implemented in areas where patients will first present: triage areas, the registration desk at the clinic or the emergency department.
Guards at the gate should wear surgical masks and maintain hand hygiene. The conversation should be carried out from a distance of at least 1 metre21.
Alternate seats can be strapped down the middle with string or tape to ensure distance seating.
Waiting in a vehicle is safer than waiting in a clinic.
Every ultrasound environment is different1. It is unlikely that ultrasound clinics have too many choices in ventilation/air conditioning. It is recommended that single unit air conditioning should be run in an “open to outside air” mode (vent open). Clinics will have to decide individually how best to facilitate maximum air change in routine practice. Aerosol generating procedures (AGP) are rare in daily ultrasound practice and should be handled by standard operating procedures by various guidelines1,2. However such AGPs should not be attempted in an ultrasound clinic but in designated centers.
All indoor areas such as entrance lobbies, corridors, and staircases, escalators, elevators, security guard booths, office rooms, meeting rooms, pantries, and cafeteria should be mopped with a 1% sodium hypochlorite solution or phenolic disinfectants. Annexure 1 shows details of how to prepare a 1% sodium hypochlorite solution and has been issued by the Ministry of Health and Family Welfare, Government of India18. Phenolic compounds are available as readymade house detergent products in the Indian market. The frequency of mopping will depend on the footfall. At 2X3 patients an hour, 2 hourly mopping is recommended. Mopping should also precede the start of work and should also be done after the last patient has departed. Cleaning should be started from cleaner areas and then proceed to dirtier areas. Cleaning staff must wear surgical masks and heavy-duty gloves. Goggles are required only if there is a risk of chemical or organic splash (WHO Rational and Appropriate use of PPE). Appropriate hand hygiene should be practiced.
High contact surfaces such elevator buttons, handrails/handles and call buttons, escalator handrails, public counters, intercom systems, telephones, printers/scanners, and other office machines should be cleaned twice daily by mopping with a linen/absorbable cloth soaked in 1% sodium hypochlorite.
Frequently touched areas like tabletops, chairs, chair handles, pens, office files, registers, keyboards, mouse, mouse pad, tea/coffee dispensing machines, etc. should especially be cleaned. These can be cleaned with 1% sodium hypochlorite or a sanitizer that contains at least 60X70% alcohol.
Metallic surfaces like door handles, security locks, and keys cannot be adequately cleaned with sodium hypochlorite and a 60X70% alcohol sanitizer can be used to wipe down these surfaces.
Sanitizing spray should not be used on potentially highly contaminated areas such as registration counters as it may create splashes that can further spread the virus. A wipe is more effective
Cleaning equipment should be rinsed in running water or hot water after use and left to dry.
Hand sanitizing stations should be installed near the entry and near high contact surfaces such as clinic registration counters
Toilet floors, toilet pots, toilet seats and lids, toilet sinks and toilet soap dispensers should be cleaned with 1% sodium hypochlorite or a phenolic detergent three to four times a day. Taps and metallic surfaces should be cleaned with a sanitizer containing 60X70% alcohol.
Outdoor areas have less risk than indoor areas because of air currents and exposure to sunlight. Cleaning and disinfection efforts should be targeted to frequently touched surfaces such as tables and bench handles.
Patient examination tables must be covered with sheets (and pillow covers if necessary) that must be changed after each patient. Linen may be disposable as per individual choice. Routine machine-washing with a regular detergent is adequate for nondisposable sheets and pillow covers. Mattresses and table edges must be sanitized using a sanitizer containing 60X70% alcohol if abundantly available or a 1% sodium hypochlorite solution.
Equipment Sanitation
SARSCoV2, the causative agent of COVIDX19 can be present on surfaces for several days.
Surfaces that come into contact with the patient (cable and transducer), as well as surfaces that are touched by the clinician (keyboard, touchscreen, trackball, handlebars, etc.), should be disinfected after each examination.
high-level disinfection (HLD) is not required when using ultrasound probes on intact skin. There is no evidence that HLD offers benefits for disinfection from SARSXCoV2.
The following steps should be followed
Excess ultrasound gel on the transducer should be wiped off with a soft cloth after each examination. Gel can harbor a lot of germs and its presence prevents adequate disinfection.
Transducer surfaces and cords should be wiped with an equipment vendor-approved low-level disinfectant (LLD). Commonly approved agents include 70% Alcohol, Ammonia, 10% Bleach, Clorox, standard dilute Cidex, Protex wipes, SaniCloth, PI Spray, Oxivir wipes, Mikrobac, Microzide, Lonza, Klercide 70 and Descocept wipes.
Equipment desktop, edges, keyboard, transducer resting stands and especially the side in close proximity to the patient should be wiped with an LLD.
Commercial wipes should not be reused. These should be disposed of in appropriate bins. Cloths may be laundered with standard machine washing.
Transducer and cord covers are too overpriced for general use. Makeshift covers like laparoscopy camera covers are difficult to source. These are not encouraged and LLD is adequate.
Ultrasound machines in COVID designated centers must be used with machine covers and covers for the transducer and cable. High-level disinfectants (HLD) is recommended in areas if ultrasound has been done where AGPs were performed. Details for COVID designated centers are beyond the scope of these guidelines.
Accelerating Availability of Final Reports
Adequate staff must be available to accelerate the preparation of reports. Lockdown conditions do not permit courier services and repeated travel. Reports and Images may be communicated by email/website access.
Advance Resourcing of Protective Devices and Materials
Pandemic conditions are traditionally accompanied by shortages. All attempts should be made to ensure adequate stock.
Staff Considerations and Education
Chronologically
older (greater than 60 years) staff or those with cardiac disease, pulmonary
disorders etc should be allocated work in areas where they have limited patient
contact or may avoid working at all.
Staff may be rostered to shorter working
hours and work in rotation.
Staff must be trained in and given appropriate personal protective equipment and encouraged frequent hand washing.
Hands should be washed with regular soap and water for at least 20 seconds.
The staff must be trained for Phone scheduling, the first point of contact interviews, documentation of demographic details and patient history, obtaining informed consent, hand washing, social distancing and donning and doffing PPE.
Concluding Comments
The basic principles8 in a situation of the pandemic are:
Resources should be prioritized and optimized.
The emphasis should be on avoiding unnecessary exposure of healthcare personnel to (potentially) infected patients and vice versa.
The number of visits should be reduced to the essential minimum.
It is wise to consider colleagues, staff, and patients as asymptomatic carriers and follow PPE measures.
Poon LC, Abramowicz JS, Dall’Asta A, Sande R, Ter Haar G, Maršal K, Brezinka C, Miloro P, Bassel J, Westerway SC, AbuXRustum RS, Lees C. ISUOG Safety Committee Position Statement: safe performance of obstetric and gynecological scans and equipment cleaning in the context of COVIDX 19. Ultrasound Obstet Gynecol 2020. DOI: 10.1002/uog.22027.
Poon LC, Yang H, Lee JCS, et al. ISUOG Interim Guidance on 2019 novel coronavirus infection during pregnancy and puerperium: information for healthcare professionals [published online ahead of print, 2020 Mar 11]. Ultrasound Obstet Gynecol. 2020;10.1002/uog.22013. DOI:10.1002/uog.22013 .
Report of the WHOXChina Joint Mission on Coronavirus Disease 2019 (COVIDX 19) (www.who.int)
Zhang Z, Liu S, Xiang M, Li S, Zhao D, Huang C, Chen S. Protecting healthcare personnel from 2019XnCoV infection risks: lessons and suggestions.
Front Med. 2020 Mar 23. DOI: 10.1007/s11684X020X0765Xx. Online ahead of print.
Yang H, Wang C, Poon LC. Novel coronavirus infection and pregnancy. Ultrasound Obstet Gynecol 2020; 55: 435X437
Wong J, Goh QY, Tan Z, Lie SA, Tay YC, Ng SY, Soh CR. Preparing for a COVIDX19 pandemic: a review of operating room outbreak response measures in a large tertiary hospital in Singapore. Can J Anaesth. 2020 Mar 11: 1–14.
DOI: 10.1007/s12630X020X01620X9 [Epub ahead of print]
Abu Rustum RE, Akolekar R, Sotiriadis RA, Salomon LJ, Da Silva Costa F, Wu Q Frasca T, Bilardo CM, Prefumo F, Poon LC. ISUOG Consensus Statement on the organization of routine and specialist obstetric ultrasound services in the context of COVD19.Ultrasound Obstet Gynecol 31 Mar 2020 doi.org/10.1002/uog.22029
Coronavirus disease 2019 (COVIDX19) pandemic: increased transmission in the EU/EEA and the UK – seventh update 25 March 2020 (www.ecdc.europa.eu)
European Centre for Disease Prevention and Control (ECDC), 2020. Infection Prevention and Control For the Care of Patients With 2019XnCoV in Healthcare Settings [www.ecdc.europa.eu/sites/default/files/documents/COVIDX19XguidanceX wearing and removingXpersonalXprotectiveXequipmentXhealthcareXsettingsX updated.pdf]
Patel A, Jernigan DB; 2019XnCoV CDC Response Team. Initial Public Health Response and Interim Clinical Guidance for the 2019 Novel Coronavirus Outbreak X United States, December 31, 2019XFebruary 4, 2020 [published correction appears in MMWR Morb Mortal Wkly Rep. 2020 Feb 14;69(6):173]. MMWR Morb Mortal Wkly Rep. 2020;69(5):140–146. Published 2020 Feb 7. DOI:10.15585/mmwr.mm6905e1
Ong, Sean Wei Xiang, et al. “Air, surface environmental, and personal protective equipment contamination by severe acute respiratory syndrome coronavirus 2 (SARSXCoVX2) from a symptomatic patient.” JAMA (2020)
COVIDX19: Guidelines on disinfection of common public places including offices (www.mohfw.gov.in)
Cleaning and Disinfection for Community Facilities: Interim Recommendations for U.S. Community Facilities with Suspected/Confirmed Coronavirus Disease 2019 (COVIDX19) (www.cdc.gov/coronavirus/2019Xncov)
Australian Government Department of Health: Environmental cleaning and disinfection principles for COVIDX19 (www.health.gov.au)
Rational use of personal protective equipment for coronavirus disease (COVID-19): interim guidance. (https://apps.who.int/iris/bitstream/handle/10665/331498/WHO-2019- nCoV-IPCPPE_use-2020.2-eng.pdf)
Annexure1:
Annexure 2:
Patient Demographics,
Declaration and Consent Form
Name &
Address of Medical Organisation Patient name: